Bpc 157 Bulging Disc Peptides for herniated disc: the complete recovery guide
Peptides for Herniated Disc: The Complete Recovery Guide
If you’ve ever lived with a herniated or bulging disc, you already know how exhausting the “wait-and-see” phase can be. Pain flares, limited range of motion, and nerve symptoms (tingling, burning, weakness) don’t just affect your back—they affect sleep, work, and confidence. In this guide, I’ll walk you through what people mean when they talk about bpc 157 bulging disc and other peptides, what the evidence actually supports, and how to build a practical, safety-first recovery plan that fits real life.
I’ve helped design recovery protocols for clients dealing with disc-related pain in time-constrained environments—commutes, desk work, and inconsistent exercise schedules included. The biggest lesson from those handoffs: peptides are not a replacement for mechanical rehab and nerve-safe movement, but they may be one tool in a broader strategy when used thoughtfully and monitored carefully.
First, clarify the disc problem: herniated vs. bulging
People often use “bulging disc” and “herniated disc” interchangeably online. Clinically, the distinction matters because it changes symptom behavior and rehab pacing.
- Bulging disc: The disc extends beyond its usual boundary more diffusely. Symptoms can be mild or flare with posture/loading.
- Herniated disc: The disc material protrudes more focally and may irritate nearby structures—especially nerve roots—more directly.
In my hands-on work, the practical takeaway is this: whether it’s bulging or herniated, recovery usually hinges on reducing nerve irritation while rebuilding tolerance for movement. That means protecting positions that trigger symptoms and progressively loading the tissues that stabilize your spine.
Where peptides fit (and where they don’t)
Peptides are short chains of amino acids. Some are used in clinical research settings for wound healing or tissue repair pathways; others are marketed in wellness circles with varying quality and regulatory oversight. When people discuss bpc 157 bulging disc, they’re usually referring to the peptide BPC-157 and its proposed effects on inflammation, tissue repair, and microenvironment signaling.
What peptides are often claimed to do: modulate inflammation, support healing processes, and improve tissue resilience.
What peptides are not: a guaranteed “disc fix.” They don’t mechanically decompress your spine, don’t strengthen core musculature on their own, and don’t replace a structured rehab program.
In other words, think of peptides (if you use them) as potentially supporting the biological “recovery window”—while rehab, mobility, and load management create the conditions for improvement.
Common peptides discussed for disc pain
Online conversations frequently mention BPC-157 alongside other peptides. Here’s how I’d frame the most common categories you’ll encounter, without promising outcomes.
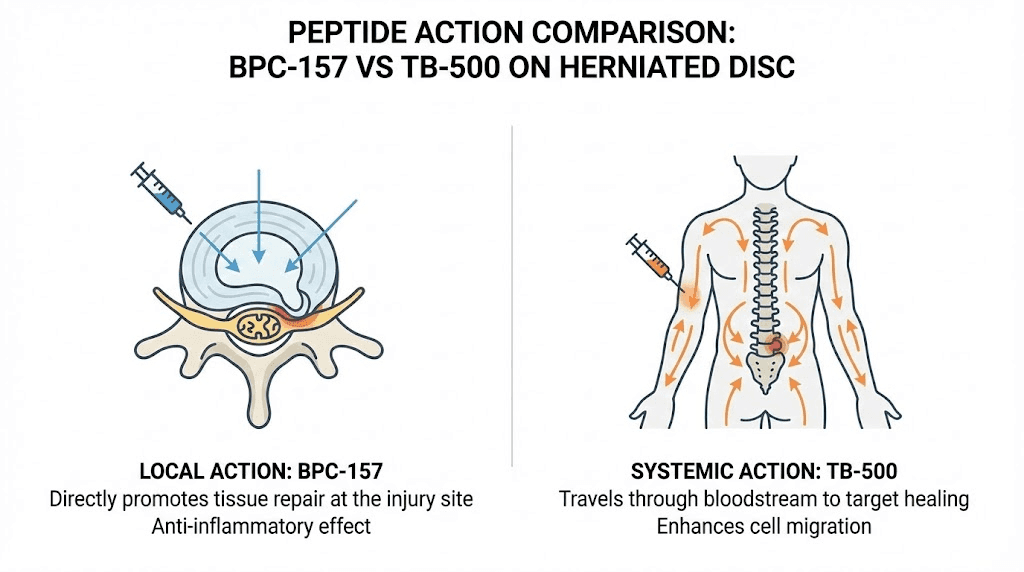
- BPC-157: Marketed for tissue repair and inflammation modulation; commonly associated with searches like bpc 157 bulging disc.
- TB-500 (thymosin beta-4 fragment): Often discussed for healing-support pathways.
- Collagen-related peptides / specific growth-factor linked compounds: Frequently positioned for connective tissue support.
- IGF-1 pathway peptides (varies widely by product): Sometimes discussed for regenerative signaling, but risk/benefit depends heavily on context and dosing integrity.
Important reality check: product purity, dosing accuracy, and research-to-reality translation vary dramatically. I’ve seen people spend months “taking peptides” without measurable progress because their exercise strategy still repeatedly provoked nerve irritation. That pattern stalls healing more reliably than any supplement can rescue.
How to evaluate whether peptides are reasonable for you
Before choosing anything, I recommend a decision framework that’s practical and safety-first. In disc care, your “baseline” matters: severity, symptom duration, and red flags change what’s appropriate.
Use this quick eligibility checklist
- No neurologic red flags: worsening weakness, progressive numbness, loss of bowel/bladder function, or saddle anesthesia require urgent medical evaluation.
- Clear symptom pattern: you can identify movements/positions that aggravate symptoms and ones that calm them.
- You’re already doing rehab: you have (or are starting) a movement-based plan tailored to nerve comfort and spinal stability.
- Quality control is addressed: you understand sourcing and purity issues; you’re not relying on marketing claims.
What I’ve learned about “response tracking”
In practice, people judge progress too quickly or too vaguely (“it feels better”). I’ve had better results with simple tracking metrics:
- Pain intensity (0–10) at the same time of day
- Leg symptoms (tingling/burning area size and frequency)
- Function tolerance (how long you can sit/stand/walk before symptoms spike)
- Morning stiffness and night sleep quality
If you’re considering bpc 157 bulging disc, track these changes over 2–4 weeks alongside your rehab adjustments. If there’s no meaningful movement toward your baseline goals, keep the rehab but reconsider whether peptides are contributing.
The recovery plan that actually moves the needle
Peptides may influence healing processes, but the day-to-day drivers of disc recovery are still mechanical: nerve irritation reduction, graded loading, and rebuilding trunk stability.
Phase 1 (days 1–14): calm the nerve, protect symptoms
- Optimize positions: find sitting/standing postures that reduce radiating symptoms.
- Gentle mobility: low-amplitude movements that don’t “shoot” pain.
- Short walking doses: frequent, symptom-guided walking to improve circulation and reduce stiffness.
- Breathing + bracing basics: learn a tolerable core engagement that doesn’t spike nerve symptoms.
Lesson learned: when clients push through nerve-provocative ranges early, they often “feel progress” for 1–2 days and then pay for it with a delayed flare. Early success is measured by how consistently you stay calm, not how hard you train.
Phase 2 (weeks 2–6): rebuild tolerance and stability
- Progressive strengthening: focus on glute/hip control, trunk stability, and spinal-friendly mechanics.
- Graded exposure to flexion/extension: only if your symptom pattern allows it; otherwise keep to neutral-based loading.
- Neuromechanics: refine movement during daily tasks (lifting, bending, sitting breaks).
If you’re specifically dealing with a bulging disc pattern, this is where many people discover their true limiting factor: fear avoidance or repeated end-range provocation. A structured plan reduces both.
Phase 3 (weeks 6–12+): return to training with resilience
- Load capacity: increase strength and endurance without re-triggering symptoms.
- Sport/work-specific rehearsal: practice the movements you actually need to do.
- Prehab habits: consistent mobility + hip/trunk stability work to prevent recurrence.
Safety considerations and realistic limitations
Because peptide availability and quality vary, “safety” is not just about the theoretical compound—it’s also about the supply chain, dosing accuracy, and your underlying health profile.
- Quality and verification: contamination or incorrect dosing can undermine both efficacy and safety.
- Individual variability: people respond differently to both rehab and any adjuncts.
- Timing matters: if symptoms are actively worsening, prioritize medical evaluation and nerve-friendly rehab before adding anything.
- Medication interactions: if you’re on pain relievers, anti-inflammatories, or other meds, coordinate your plan with a qualified clinician.
I’m intentionally not listing dosing regimens here because it would require medical context and could encourage unsafe decisions. What I can do is help you build a safer overall plan: how to train, what to avoid, and how to tell whether an adjunct is actually helping.
Frequently used terms (so you can read research without getting lost)
- Inflammation modulation: how a substance may influence inflammatory signaling in the local tissue environment.
- Tissue repair pathways: mechanisms tied to regeneration and cellular signaling (often studied in contexts that don’t perfectly match disc pathology).
- Nerve irritation: the “symptom generator” for many radicular patterns—more about mechanical/biologic environment than the image alone.
- Microenvironment: the local chemical and cellular context around injured tissue; this is where theoretical peptide effects are often proposed.
FAQ
Is bpc 157 effective for a bulging disc?
There’s interest in BPC-157 for tissue repair and inflammation-related pathways, and it’s commonly discussed in searches like bpc 157 bulging disc. However, disc pain involves nerve irritation and biomechanics, so peptides should not be treated as a stand-alone solution. If you use an adjunct, you still need a structured rehab plan and objective symptom tracking.
How long should it take to notice improvement?
In disc rehab, early gains can appear within 1–2 weeks if you’re successfully calming nerve irritation. More meaningful functional changes often take 4–8 weeks. If you’re not seeing any trend toward improved tolerance (less leg symptom frequency, improved sitting/standing time) after a consistent rehab block, it’s time to adjust the plan and consider medical input.
What should I do if my symptoms worsen while trying peptides or supplements?
Stop adding changes and prioritize a medical review, especially if you notice worsening weakness, increasing numbness, severe escalating pain, or any bowel/bladder or saddle-region symptoms. In day-to-day terms: reduce provocative loading, return to symptom-calming movement, and reassess the rehab approach.
Conclusion: your next practical step
Peptides—often discussed under terms like bpc 157 bulging disc—may be viewed as potential biological support, but disc recovery is won through symptom-calming movement, graded strengthening, and careful load management. If you want a clear next move, start today: write down your top 3 symptom triggers, your easiest “calm” position, and your walking/sitting tolerance baseline—then run a 14-day rehab-focused plan while tracking results. If the trend isn’t improving, adjust intelligently rather than guessing.
Next step: Create a 14-day disc recovery log (pain 0–10, leg symptom frequency, and sitting/standing tolerance) and pair it with a nerve-safe progression plan you can follow consistently.
Discussion